PCI of anomalous Circumflex artery from Single Coronary Ostium
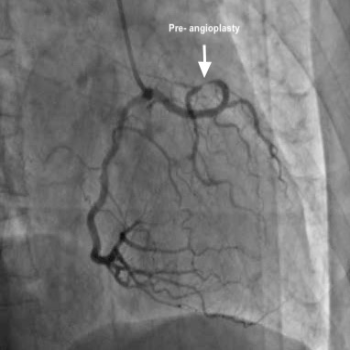
A 72 yr old gentleman (Mr Peer Mohammed) with history of anginal chest pain had undergone a coronary angiogram in Oct 2017 in a large institute in Bangalore (NH). His coronary angiogram showed single ostium coronary artery (only one artery coming from aorta) from the right sinus with RCA and anomalous Cx coming at the same ostium. An aortogram showed absent LAD artery. His anomalous Cx artery has severe mid vessel stenosis of 90%. He was told it is a complex procedure to treat with angioplasty and was put on medical therapy despite typical anginal history with chest pain on minimal exertion. He was also known to have CKD with Creatinine of 2 mg/dl.
He came to see me with the angio CD and symptoms in May 2018 for the first time. I reviewed the angiogram and mentioned that I am able to do angioplasty for him, even though it is complex- but with special techniques. His creatinine was also noted to be high (2 mg/dl), therefore the contrast load should also be minimised. He agreed and got admitted on 4th June 2018. I performed his angioplasty of his anomalous Cx artery arising from single coronary ositum via radial approach on 5th June 2018. I used a special mother-and- child catheter to reach the lesion and to reduce the amount of dye usage- managed to use only 50 ml of contrast. The procedure went successfully with deployment of 1 stent and good flow. He was discharged on 7th June 2018 and his creatinine on discharge date was 1.58 mg/dl.
This is a rare case of stenosis in anomalous circumflex artery arising from single coronary ostium. The risk of this procedure is higher than LMCA angioplasty as the patient’s heart is getting blood supply from only one limb- which divides into two. Any damage to the main limb will cause sudden cardiac arrest, therefore the procedure should be done with utmost care to avoid complication.